Teacher Education: How teachers can work on improving students’ health in schools
Good health and nutrition can promote learning and ensure that the student is ‘present, ready, and able to learn’, a foundational requirement for achieving India’s goal of Education for All, writes Shreelata Rao Seshadri in the Learning Curve magazine.
Importance of good nutrition for children
Imagine a young child in a typical government school in India. This little girl is six years old and getting ready for school. Her mother is getting ready too because she must be in the field by 7 am. She has no time to make breakfast for the little girl or her brother. The little girl barely has time to wash her face and get into her school uniform.
There is a bit of rice leftover from the night before, which the mother hurriedly divides between her two children – barely a mouthful each. Then, they run to school, just in time for the assembly. As they file into their classrooms for their first lesson, the little girl feels a familiar rumble in her stomach – she is hungry, and lunch is several hours away. It is going to be another long morning.
This is the reality for an estimated 25 million children in India. There is substantial evidence that the nutritional outcomes of school children are at considerable risk and need urgent attention. Nutrition during school-age is critical for several reasons: it is not only of intrinsic value in terms of the child’s physical health and sense of well-being; but also, of instrumental value in terms of improving the child’s learning outcomes and leading to better employment prospects in the long run.
Over a lifetime, every additional year of education has been shown to increase lifelong earnings by 20%. Yet, malnutrition continues to be a serious problem in India, particularly among school-age children (Table 1).
For those belonging to poor families, who constitute the majority of children attending government schools, close to 30% are likely to suffer both low height-for-age and weight-for-age, as well as high rates of anaemia.
Table 1: Malnutrition among school-age children
| Poorest | Poor | Middle | Rich | Richest | Total | |
|---|---|---|---|---|---|---|
| Children age 5 – 9 years who are stunted | 30.3 | 26.2 | 22.2 | 18.4 | 12 | 21.9 |
| Children age 10 – 19 years with low BMI | 27.2 | 26.6 | 26 | 22.2 | 18.2 | 24.1 |
| Children age 5 – 9 years with anaemia | 30.1 | 29.2 | 22.4 | 18.2 | 18.1 | 23.5 |
| Adolescents age 10 – 19 years with anaemia | 33.4 | 29 | 28.4 | 28.6 | 23.1 | 28.4 |
| 5 – 9 year-olds with Vitamin D deficiency | 13.3 | 13.2 | 14.8 | 20.4 | 30.2 | 18.2 |
| Adolescents with Vitamin D deficiency | 18.9 | 18.8 | 19.8 | 28.7 | 32.9 | 23.9 |
Source: Comprehensive National Nutrition Survey (CNNS) 2016 – 18
* Stunting denotes low height-for-age
** BMI stands for Body Mass Index and is a measure of weight-for-age
*** Anaemia denotes iron deficiency
The foundations of physical and cognitive development of children are laid when the mother is pregnant and in the first 24 months of life. In this period (the first 1,000-day window), under-nutrition and/or micronutrient deficiencies can impair child development irreversibly.
Similarly, among school children and adolescents, normal growth and development are determined by several factors such as adequate nutrition as indicated by normal weight or height-for-age, absence of nutritional deficiencies (especially micronutrients like iron and iodine), a robust immune system capable of protecting against repeated illness, and the ability to participate cognitively and socially in the learning process.
School-based nutrition and health interventions, such as the provision of macro- and micro-nutrients, clean drinking water and sanitation facilities and health and nutrition education, are meant to address critical contributors to better health and learning outcomes. Such interventions, if implemented comprehensively and well, will have far-reaching positive consequences.
Recognising nutritional problems in class
Classroom hunger is a well-recognised phenomenon and it hurts the child and the learning process. Watch out for some of the following signs and symptoms of a hungry child:
- Tiredness and irritability, heightened anxiety
- Lack of energy
- Inability to concentrate
- Always feeling cold
- Depression, sadness, tears
- Disinterest in socialising, aggression, disruptive behaviour
- Falling sick often, or taking a long time to get better
- Lack of growth, low body weight, visible loss of muscle or fat
- Learning difficulties
Various factors contribute to malnourishment in children, such as:
- Extreme poverty and other socio-economic factors such as land ownership and mother’s education which determine the adequacy and diversity of household food consumption.
- Disease prevalence due, largely, to the lack of clean water and sanitation, causing repeated episodes of ill-health and thereby, impacting nutritional outcomes.
- Lack of community knowledge and awareness about a child’s nutritional requirements.
- Poor implementation of government programmes, as a result of which children lack access to a balanced diet.
Not all these issues can be addressed by the school. But in the next section, we will explore some things a school can do to promote the nutritional well-being of its students.
What can you do?
The ‘Whole School Approach’
It is critical that the school addresses the nutritional needs of children in a systematic, equitable, and sensitive manner. The World Health Organisation (WHO, 2006) advocates the ‘whole school approach’ for this.
Briefly, it is an attempt to bring together all the stakeholders involved in the health and nutrition of the child and engage them actively. This includes not only the school teachers and others who provide the meals (cooks, helpers) but also the child’s family, community, local panchayat, and frontline health workers.
Figure 1 illustrates the ‘whole school approach’.
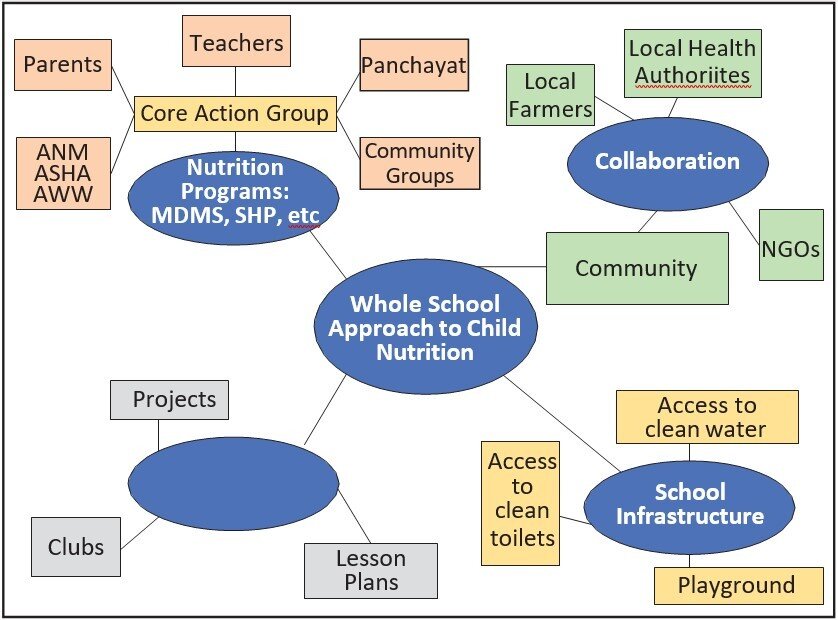
Figure 1: ‘Whole school approach’ to child nutrition
Source: Adapted from Sustain 2005 (ref. Food and Schools, WHO 2006; p.10).
Following this approach, there are several steps to improving health and nutrition in your school.
Assemble a core action group
Many schools already have a School Development and Monitoring Committee (SDMC). This is the Core Action Group since the membership includes diverse stakeholders. However, the SDMC is often not active and meets rarely.
Ensuring that the SDMC meets regularly is critical and a particular day, every month should be set aside for this. The agenda can cover infrastructure and maintenance (toilets, water supply), student welfare and implementation of government programmes.
Two programmes that require close monitoring are:
- The Mid-Day Meal Scheme (MDMS): The MDMS provides a hot, cooked meal for all primary school children from classes I‑VIII. The objective is to provide children with a balanced and nutritious diet to combat classroom hunger and it includes rice or chapati, along with some type of dal and vegetables.
The rice or wheat is supplied directly to the school by the government. But dal and vegetables have to be purchased by the school with the allowance per child provided by the government – usually a meagre amount.
The SDMC can enrich the meal by accessing funds from the panchayat or in-kind assistance from the community. There are examples of community members or local farmers providing seasonal vegetables either free or at reduced costs, or a morning snack of peanut chikki or fruit (bananas, guava or papaya are local fruits high in nutrients).
Or the SDMC could mobilise community mentors to help the students to develop a vegetable garden in the school. This would supplement the vegetable budget and can also be part of the biology and/ or environmental science curriculum. - School Health Programme (SHP): The SHP provides basic health check-up for all children, along with vitamin A and iron supplementation and regular deworming.
The SDMC can coordinate with the local Primary Health Centre/ANM to ensure that the check-up and supplementation take place regularly according to the agreed-upon timelines and that Student Health Cards are maintained and updated.
This will ensure that minor ailments are diagnosed early and treated quickly, with minimal loss of school days for the child.
In addition, regular growth monitoring can be introduced to track height and weight of children and to make sure that they are not at nutritional risk.i
Ensure a working infrastructure
Water, Sanitation and Hygiene Education (WASH) in schools is a strategy that provides for clean water and sanitation facilities for all children, as well as sensitisation on why this is necessary. Children spend a significant portion of their day in school, and WASH has been shown to impact their learning, health and dignity, especially for girls (UNICEF 2018).ii
- Only about 60% of children have basic sanitation facilities (toilets) at home. The school may be the only place where they can access a clean toilet in privacy.
- While most children have access to water at home, it is of varying quality. Providing clean drinking water in school reduces their chances of illness due to water-borne diseases (typhoid, jaundice).
- Instilling the hand-washing habit, practised properly, will protect children from many infectious diseases, including COVID-19. Posters are a good way to communicate the message.iii
Other than WASH, playgrounds have a huge role in maintaining children’s well-being. Play is a positive force for social, emotional and cognitive development; it also prevents obesity, a growing problem among school children today.
Introduce nutrition into the curriculum
The school curriculum already includes lessons and activities around food and nutrition, health, hygiene and sanitation-related topics. Some of the thematic areas that could be actively brought into classroom pedagogy are indicated in the table below:
Table 2: Tentative thematic areas for intervention in curriculum for classes I‑V
| Thematic Areas | Sub-topics |
|---|---|
| Food & Nutrition | Why do children like some foods and not others? |
| Washing vegetables, fruits before eating | |
| Making juice, sprouting grains and making salad | |
| Preparing diet charts | |
| Improving MDM through a school garden | |
| Water & Sanitation | Toilet survey at school and village: who has, who uses |
| Purification of drinking water & its storage | |
| Conserving water – how to use water wisely | |
| Personal Hygiene | Hand-washing |
| Brushing teeth, rinsing mouth after eating | |
| Cutting nails | |
| Regular physical exercise | |
| Waste Cleaning | Keeping surroundings clean at school and at home |
| Using the dustbin | |
| Separating wet and dry waste | |
| Treatment | Making Oral Rehydration Salts (ORS) |
| Planting medicinal plants and using traditional medicine for basic ailments | |
| Maintaining and using the first-aid box | |
| Health Monitoring | Using a thermometer |
| Counting breathing rate, pulse rate | |
| Measuring height and weight on a quarterly basis, calculating BMI and maintaining growth chart | |
| Preparing and maintaining health cards | |
| *Conducting eye check-up using a Snellen chart |
This table was developed by the Health, Development and Society team in collaboration with the Work and Education team, based on a careful review of Government of Karnataka textbooks and the literature on global evidence of successful initiatives in schools.
Note: *These sub-topics are not in the textbooks but are included because they are linked with malnutrition.
Build relationships with community
The community is invested in the health and well-being of their children since most families have children attending the school. Reaching out to the community for support not only widens the umbrella of resources available to the school, but also promotes ownership of the school and its success within the community.
Providing additional food, either regularly or as occasional treats, volunteering their time during the lunch hour to ensure that all children eat well, taking them outdoors for fun and exercise, teaching them how to grow or sprout or cook vegetables – these are all ways in which community members can contribute to the children’s health and nutrition.
Conclusion
Ultimately, the health of the school-going child is a joint responsibility: it is the responsibility of the government to provide critical services to support his or her mental and physical well- being, it is the responsibility of the community to hold the government accountable for quality and transparency and it is the responsibility of the parents to ensure that their children are well-fed and cared for.
However, the school plays a central role in ensuring that the services children need, reach them. This is important for several reasons:
- It extends the benefits of early childhood health and nutrition programmes, for example, the Integrated Child Development Scheme.
- Nutrition services can be delivered efficiently in schools since so many children gather in one place.
- Evidence shows that good health and nutrition promote learning – the school’s central purpose. Most importantly, school health and nutrition programmes ensure that the student is ‘present, ready, and able to learn’,iv a foundational requirement for achieving India’s goal of Education for All.
About the author:
Shreelata Rao Seshadri has been involved in research, practice and teaching in the field of public health for almost three decades. She has had a range of professional engagements, including with multilateral agencies, global research initiatives and grassroots NGOs.
Her research interests are largely focused on health policy and systems research, with a special interest in program implementation and evaluation.
Shreelata has published widely on a range of public health issues, including nutritional challenges faced by primary school children, traditional food systems and their transformation, and governance issues associated with access to health and nutrition services in both urban and rural settings.
Subscribe to Learning Curve
Click here to read the full issue of Learning Curve →
Click here to read all issues of Learning Curve →
Know more about Azim Premji University’s Master of Public Health programme here.